The 56th Forum offers opportunities to explore the cinema status quo in all its many facets and shows films by people who take their work and its impact seriously: the way it affects our coexistence, our battles, our reconciliations, our history and stories.
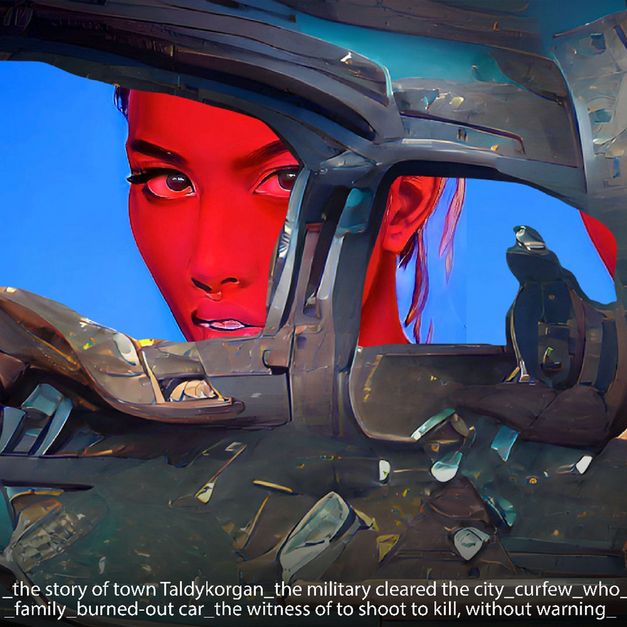
In Forum Special, we reflect on current social and political questions. The short film programme AI Realism and the accompanying discussion event “Solidarity Algorithms?” examine what the promise of empowerment through AI tools amounts to in the face of economic, political, and sexist violence.
Forum Special also dedicates a programme to the recently deceased Hungarian director Judit Elek, featuring the documentary ISTENMEZEJÉN 1972–73-BAN (A Hungarian Village) and the short film TALÁLKOZÁS (Encounter).
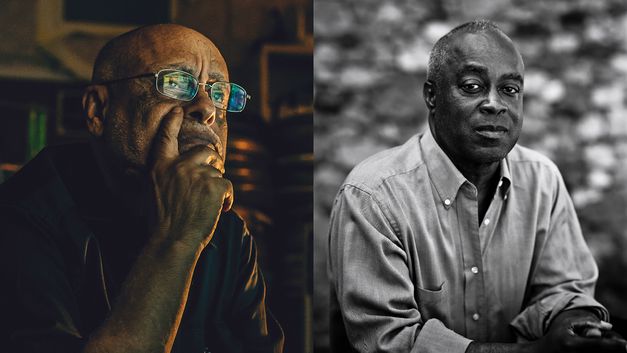
In a discussion event, two legends of Black cinema, Charles Burnett and Haile Gerima, come together to talk about Hollywood and cinema in the face of racism, fascism, and colonialism, then and now.
And last but not least: the TEDDY Award turns 40! In the special programme TEDDY 40, we are screening VERFÜHRUNG: DIE GRAUSAME FRAU (Seduction: The Cruel Woman) by Elfi Mikesch and Monika Treut, which was shown in the Forum in 1985.